

In addition to being the MLA for our North Island riding, Dr. Anna Kindy is also the Health Critic for the Conservative Party of British Columbia. She recently had a conversation with Cortes Currents about the state of healthcare in British Columbia.
Anna Kindy: “That portfolio has kept me quite busy, to be honest. There are issues throughout British Columbia, like we’ve heard on the news. I have my tentacles in all sorts of health authorities, and people are communicating with me from the front lines.”
“When we’re looking at healthcare right now, it probably will be getting worse before it gets better unless we start shifting. What we’re seeing is that issues with accessing primary care are still a big issue for people. There are issues with accessing specialty care. The Consultant Specialists of BC put out that 1.2 million people are on a waitlist right now. Just to give you an example of what specialists need to do now—for example, in neurology—they get so many referrals that they need to triage what is important, what needs to be dealt with right away, and what doesn’t, because they can’t keep up. What happens is some people end up getting worse as they’re waiting. Over 4,600 British Columbians have died waiting for care.”
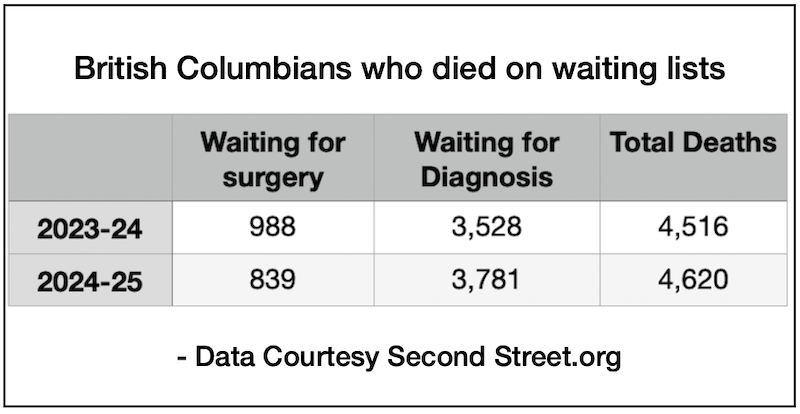
Cortes Currents: According to the 2025 ‘Died On A Waiting List‘ report, 839 British Columbians died while waiting for surgery and another 3,781 died while waiting to be diagnosed.
Anna Kindy: “Over 25,000 British Columbians have gone outside BC to get care. The other thing we’re seeing as well is access to emergency departments. In Port Hardy, the emergency department is still not open after five PM. We’re going on three years now, open from morning till five o’clock, and that causes a domino effect. When an emergency closes, people have to go to the closest hospital, and it’s stretched thin already.”
“We’re seeing these emergency closures across the province. The ministry will say it’s getting better, but the numbers are still completely unacceptable. I’ve never seen anything like it.”
“The other issue is what I call emergency block. Many hospitals are run over census. For a hospital to be safe, it should be under 95% capacity, and even that is stretching it. Many hospitals across the province are running over that. For example, our own hospital in Campbell River. Our hospital was built in 2017 initially for 95 beds. They increased the capacity to 105 by doubling up beds, but we were running at 161 patients in a hospital that does not have the capacity for that.”
“What that means is the people in emergency are stuck in emergency. They can’t go upstairs. They’re stuck on stretchers, but also if they’re admitted, sometimes they’re on stretchers in family rooms or in the hallways.”
“We’re seeing that across British Columbia. In our own Campbell River Hospital, my husband was part of the administration for the transition, and everyone was saying you need to have at least 150 beds. Just looking at the demographics and the growth, we need at least 150 beds. So here we are with much less than that.”
“The other concerning thing, and I’ll be specific to my riding, is that we were promised a long-term care facility. We’ve been promised that for a number of years. Regarding the estimates for the budget, they said ‘yes, it’s a goal, we’re building this long-term care facility,’ but they haven’t broken ground yet. Talking to folks on the ground, sometimes there are people stuck in the hospital for months waiting for a bed in long-term care, and then from the community, it takes up to four years to get into long-term care.”
“What I’m seeing is a failure at every level in accessing care in a timely way. So that’s where we are. People tell me, ‘Well, it’s fine and dandy showing us what’s not working, but what’s the solution to that?’”
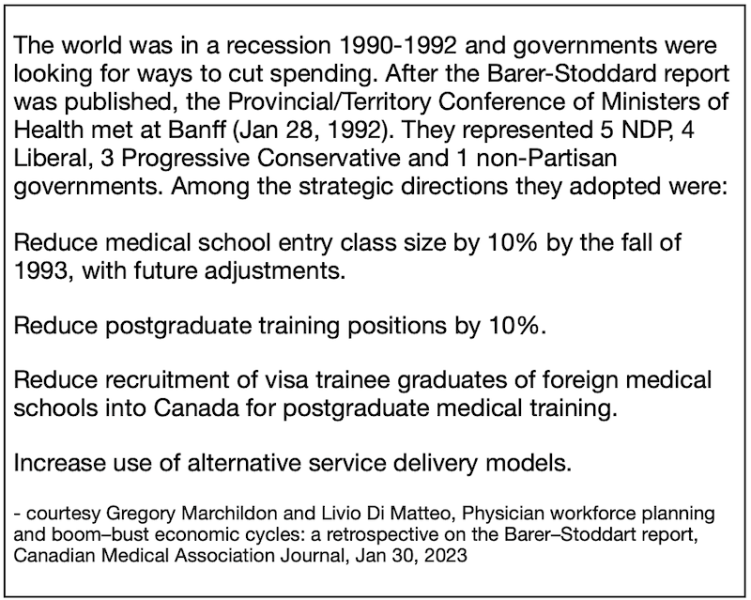
“Talking about the solution, we need to look at the historical context of why we are where we are and then go from there. So, in the early nineties, the NDP government had done a study that basically said healthcare costs were going up. What they were pointing at was too many doctors driving up the costs and too many hospital beds. Things like “a hospital bed built is a hospital bed filled” was quite the quote. So what happened was there was a cutback in the number of doctors and the number of spots in medical schools, and they also cut back on hospital beds.”
Cortes Currents: A quick search of the internet revealed that the 1991
Barer-Stoddart report was not commissioned by the BC NDP, but rather the Federal/Provincial/Territorial Conference of Deputy Ministers of Health. British Columbia was one of the provinces that ignored warnings from the Association of Canadian Medical Colleges and proceeded to cut enrolment, cap residencies and stall funding. The shortcomings of this approach were already becoming apparent before the BC Liberals took power in 2001, and shortly after the end of their 16 year tenure a study from UBC warned that BC’s serious shortage of doctors was only going to get worse.
Anna Kindy: “When we fast forward to now, the data was there to show us that we need a much higher number of doctors and number of beds, but they haven’t followed through with that. And so now what we’re seeing is a band-aid solution of trying to quickly get people certified in BC to be able to practice. I call it sometimes “poaching from overseas.” The issue I’m starting to see in certain jurisdictions is quality. We’re sometimes fast-tracking a bit too quickly and there are issues on the ground.”
“I have meetings every month with Island Health, and I had a meeting with the CEO of Island Health a bit over a month ago. We have contract issues with people from the front lines. People want to stay, they want to attract people, but they’re not moving very quickly with the contracts. So, I brought that forward. As well, we tried to brainstorm how to get more bodies in Port Hardy to have the emergency opened. I’m talking regularly with Island Health, but those are all, in a sense, what I call band-aid solutions.”
“We’re trying to make it work, but not really doing what’s needed to fix this so that it’s much better in five or ten or fifteen years. Again, we have an aging demographic in British Columbia, and second, there’s an aging demographic of physicians as well. Up to 40% of GPs will be retiring potentially in the next five years, and some of the specialties as well. So the government will say, “We’ve set up SFU with a new medical school,” but the first year has only 52 spots. I think they’re going to go up to 150, but that’s not enough. We need way more than that.”
“I think they had over 3,000 applicants for 52 spots.”
“So what’s happening is some of our really good folks in British Columbia end up going to different countries to get trained, and they have a hard time coming back. Sometimes they don’t come back because they like it where they’re at. We sometimes lose very good British Columbians to the system because we’re making it more difficult to come back because there are no spots. Or they end up going, for example, to New Zealand, where the healthcare is not where we’re at; it’s not the same type of crisis. So they sometimes can end up staying there. We’re losing good British Columbians, and so we need to train more.”
“I was talking with a group of Doctors of Osteopathy (DOs), and they are meeting the ministry this month; they finally got an appointment. I think a quarter of the doctors in the States are DOs. They do the same pre-med, the same medical training, except they do 200 extra hours of musculoskeletal work and they can go into any residency specialty.”
“There’s a school, the New York Institute of Technology, that was interested in opening a school in British Columbia, with up to 150 spots. Rather than having our British Columbians go overseas to get trained and then pay out of pocket, why not have them train here? They had a plan of how to get primary care people trained in rural places so that they actually end up staying there. I’m hoping that moves forward because we need the numbers to increase.”
Cortes Currents: Vermont has been licensing osteopathic physicians (DOs) since 1896 and they have been recognized throughout the United States since 1973.
Anna Kindy: “Basically they have two schools in the States and they’re rated 10th, I think, out of around 40 medical schools, which is quite good, and the DOs are known to be good doctors.
Cortes Currents: Do they stay in the communities where they’re trained?
Anna Kindy: Two things. I’ve seen here in Campbell River people from outside the area doing their residency here and then ending up staying here, right? Or students coming and doing a rotation through our hospitals and they like it and they end up staying. So the answer is yes.
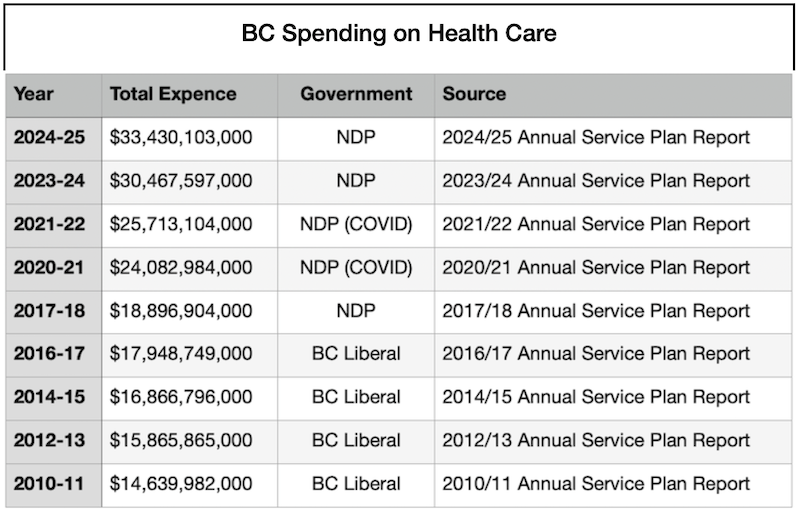
Cortes Currents: I read that 40% of the province’s total operating expenses go to healthcare. So, are we not spending that money wisely? Or do we need more money?
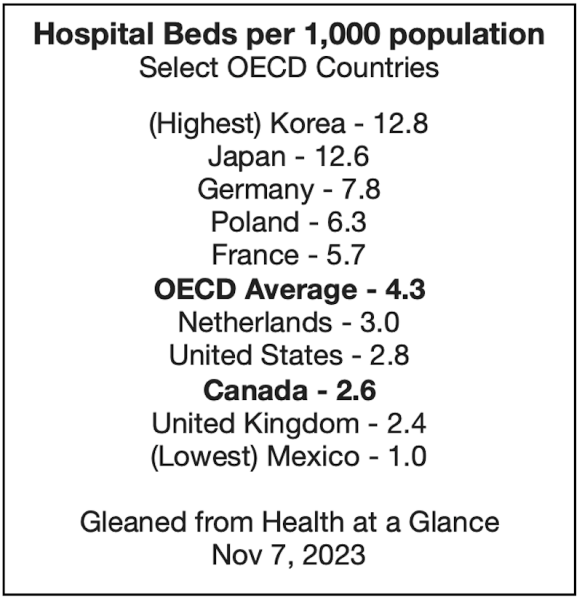
Anna Kindy: I’m going to answer this in two separate ways. We’re spending almost $40 billion in healthcare and we’ve had a bureaucracy that’s ballooned. So we are one of the higher spending OECD (Organisation for Economic Co-operation and Development) countries, and that’s 31 countries. We’re looking at all of Europe, Australia, and New Zealand. We’re one of the higher spending countries, but we’re at the bottom of the list for the number of doctors, number of hospital beds, and MRIs.”
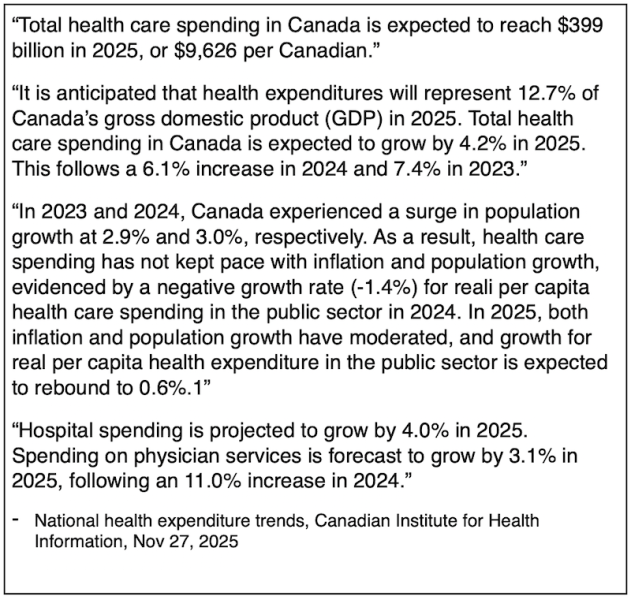
Cortes Currents: According to the Canadian Institute for Health Information, “in 2023 (the latest year for which comparable data is available), the United States had the highest ratio of health spending to GDP (16.7%). Canada (11.2%) was among a group of higher-spending countries such as the United Kingdom (11.0%), Sweden (11.3%) and France (11.5%).”
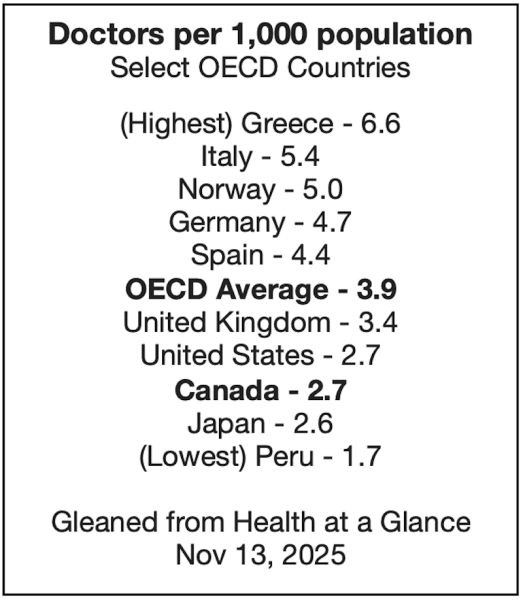
However Canada does rank below average in the OECD in terms of the number of doctorsand hospital beds.
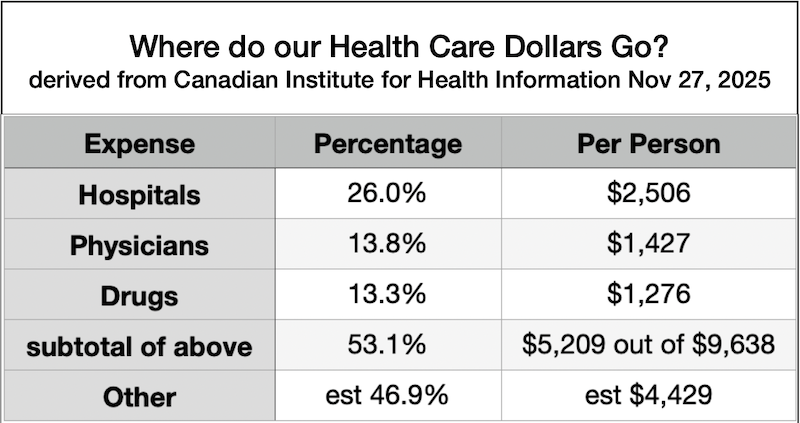
(Editor’s note: the numbers above are estimates rather than exact figures, but never-the-less suggest considerable publicity, research and administration costs. Is there a more appropriate amount for this? )
Anna Kindy: “So we need to streamline the process as one way of trying to get more money to the front lines. But to be honest, we’re not in the eighties or nineties anymore, and medicine has really evolved, and there are so many things we do now that we didn’t use to do.”
“People are living longer because of what we’re doing. So can we afford what medicine has to offer now? Even, for example, for rare diseases, drugs are extremely expensive. Can we as a society afford that? And that’s the big question. I would argue that right now we can’t, and that’s why we’re seeing rationing.”
“Even if we streamlined, I think it would be difficult to give the standard of care that some countries give that we’re not potentially giving because of the cost. This is part of what we’re seeing, and I call it rationing. When you have difficulty accessing primary care or specialty care or hospital beds, that’s called rationing.”
“We don’t have the money to build more hospitals, or if they do, is it done efficiently or not? Because government tends to be inefficient. If you compare government to a private entity, they tend to be more inefficient and it’s more costly.”
“I’ve done a deep dive into other countries and what they’re doing, and they’re doing better overall. Patient access is quite a bit better, and so that’s the discussion we need to have as British Columbians.”
“Where do we want to head from here? We need a serious discussion. When you’re talking about over 4,600 people dying while waiting; that’s not okay. Some people get an amazing journey through our healthcare system, but unfortunately, too many people are falling through the cracks.”

“In smaller communities, for example, like Cortes Island, Quadra Island and other areas, we need to make sure that you’re provided the primary care access that you need, which is becoming more difficult.”
“It’s a conversation we need to have. How do we get to where we want to get? We can’t be doing the same thing for the next two, three, or four years.”
Cortes Currents: What do you think about Medical Assistance In Dying (MAID)? I’ve both met and heard of elderly patients who very much wanted to die.
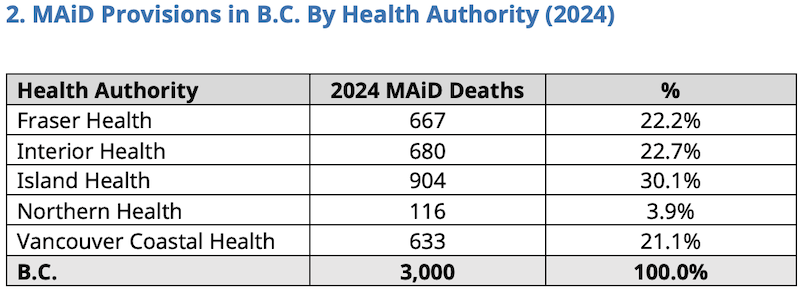
Anna Kindy: “Island Health has the highest rate of MAID in the world. We can look at it as a cost-saving measure, but I kid you not, it’s occurring when people are not accessing timely care. There were a couple of people in Campbell River that had mental health issues and pain issues, and they couldn’t access the pain clinic in Nanaimo quickly enough, and got MAID. I’m a libertarian, so it’s up to you and your doctor to decide, but on the other hand, we have to protect our vulnerable population. What I’m seeing is that we don’t have Ontario’s oversight, and we need to set up oversight to make sure that vulnerable people aren’t accessing MAID when they shouldn’t. These are stories because I’m a health critic and I hear it from other jurisdictions. For example, a patient with Lou Gehrig’s disease was asked 30 times if he wanted MAID. He clearly said, “I do not want MAID,” and to be asked 30 times is not okay.”
You have to look at depression too, and especially elderly people that are isolated. Are we taking care of our elderly people? Do we take care of each other? I think we need to have that conversation.
I have stories of relatively young people with stage four cancer that were offered MAID very quickly and they didn’t want MAID. That particular person ended up going to the States to get help because she had been in the armed forces there. She’s still alive today, but here she was offered MAID.
There’s one recent case, a young person, I think a 26-year-old, who was more or less shopping for MAID. Originally from Ontario, refused there, ended up here and utilized MAID. It was not for a life-threatening condition. When you have a mental health issue and you’re depressed—are we overstepping there?
We want to make sure that if MAID is done, it’s done for the appropriate conditions, and right now we’ve bypassed that. We need to have oversight to make sure that people who are vulnerable, especially in the midst of a health crisis where you cannot access healthcare, are protected.
Links of Interest:
- B.C.’s consultant specialists push province to reduce bloated waitlists – CTV News
- The 2025 Died On A Waiting List’ Report – Second Street.org
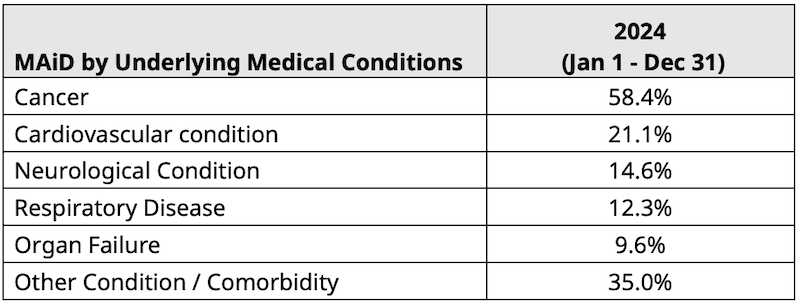
- Medical Assistance in Dying (MAID) Statistical Report 2024 – BC Ministry of Health
- Articles about, or mentioning, Anna Kindy
Top image credit: Campbell River hospital – courtesy Google Maps; MAID Charts taken from Medical Assistance in Dying (MAiD) Statistical Report
2024; All other charts by Roy L Hales using data from cited sources
Sign-up for Cortes Currents email-out:
To receive an emailed catalogue of articles on Cortes Currents, send a (blank) email to subscribe to your desired frequency:
- Daily, (articles posted during the last 24 hours) – [email protected]
- Weekly Digest cortescurrents – [email protected]